Achieving UHC- Where We Stand on NCD Care.
Universal health coverage efforts must increase focus on noncommunicable diseases.
Universal health coverage (UHC), or “health for all,” is a long-term goal for the World Health Organization and the global health community at large. UHC is defined as “all individuals and communities receiv[ing] the health services they need without suffering financial hardship.” WHO Director-General Tedros Adhanom Ghebreyesus has expressed that UHC is the “top priority at WHO.”

Even as the WHO and governments around the world have made significant progress toward this goal, it appears that access to chronic disease services has been lagging behind coverage for other essential health services, like vaccinations, access to clean drinking water, and others. This is unsurprising as resource allocation for chronic disease care has historically been insufficient, but it must be addressed as the global health community continues to work toward UHC, especially given the outsize burden of disease attributable to noncommunicable diseases (NCDs).
Despite the inclusion of NCDs on the WHO-World Bank list of key indicators for progress toward UHC, data on actual service coverage for NCDs is difficult to come by. In many cases, global health databases use proxies for NCD data, like data on risk factors, in lieu of direct data on access to NCD-related services. This is in contrast to infectious diseases and other UHC indicators, for which direct data is usually accessible. The WHO, for example, has robust data on HIV and TB service coverage, but only risk factor data for diabetes, and data on the existence or nonexistence of national screening programs for cancers.
The OECD does have limited data on actual service coverage for NCDs — namely, screening rates for breast and cervical cancers among women in OECD member states. The coverage rates for these screenings over the past 20 years are displayed in the graph below.

For purposes of comparison, the graph also displays the percentages of children vaccinated for measles and diphtheria, pertussis, and tetanus. These vaccinations and screenings are low-cost, early interventions that pay large dividends in the long-term by averting or detecting early serious, severe health conditions. While the vaccinations for communicable diseases have near-universal coverage, the cancer screenings hover around 60% and have not been trending upwards since 2000. These particular NCD and infectious disease interventions are just a few examples, but a broader look at trends in mortality from NCDs (a useful proxy for service coverage) relative to other causes points to the same phenomenon: even as the world has made progress toward UHC and reduced mortality more generally, NCDs have stubbornly remained prevalent and lethal. The figure below, drawn from the IHME Global Burden of Disease database, illustrates this disparity.

Over the past 20 years, low-income countries have seen drastic reductions in all-cause mortality, roughly halving the average mortality rate in this income category between 2000 and 2017. This trend indicates a truly remarkable improvement in health and well-being generally, surely attributable in part to efforts to advance UHC. During that same period, however, the NCD mortality rates have hardly budged. As low-income countries make massive progress in reducing the most common causes of death, they struggle to make any progress fighting NCDs. A very similar trend is observable in lower- middle income countries, as shown below.
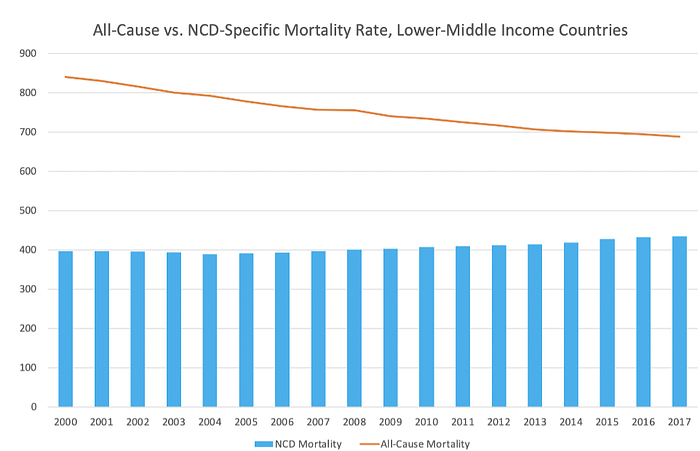
Here, the reduction in all-cause mortality is less drastic (though still quite significant), and NCD mortality rises very slightly instead of falling slightly. The graph tells the same story, though: efforts to connect people with essential health services have successfully reduced preventable deaths, except when it comes to NCDs.
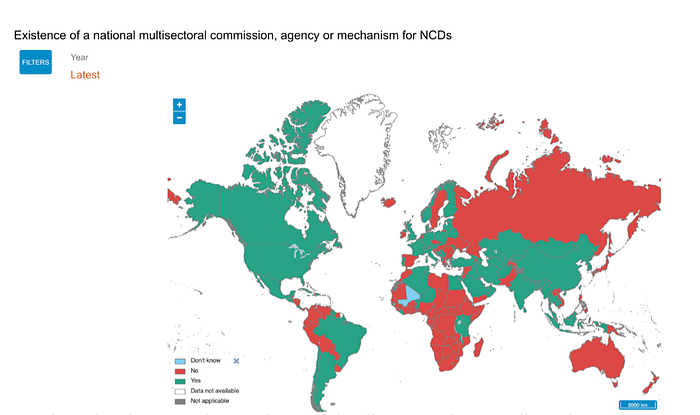
The explanation for the lack of progress on NCD coverage is relatively simple: though NCDs are the single leading cause of death (accounting for 71% of deaths annually), only 2% of development assistance funding goes toward fighting NCDs. Many low-income and developing countries still lack a national plan for combating NCDs, as shown in the following WHO graphic.
It’s clear that increased attention and funding must be contributed to NCDs as part of the WHO and other governmental and non-governmental organizations’ efforts to achieve UHC in the coming years. Especially in low-income countries, blended finance mechanisms offer promising solutions to these challenges — “simultaneously de-risk[ing] private investments and enable[ing] health initiatives to continue to scale and replicate after the exit of donor capital.” And effective investment in combating NCDs offer huge returns for the global economy, potentially averting nearly $50 trillion in healthcare costs and losses to economic productivity associated with these diseases.
